Umbilical Hernia - Diagnosis And Treatment During Pregnancy
Women are more likely than males to have an umbilical hernia. Because of the steadily increased intra-abdominal pressure, pregnancy may induce herniation or make an existing one visible.
Author:Karan EmeryReviewer:Katharine TateOct 10, 20234.1K Shares86.8K Views
Women are more likely than males to have an umbilical hernia. Because of the steadily increased intra-abdominal pressure, pregnancy may induce herniation or make an existing one visible. An umbilical hernia occurs in 0.08 percent of pregnant women. The surgical protocol for a pregnant lady with a hernia is unclear.
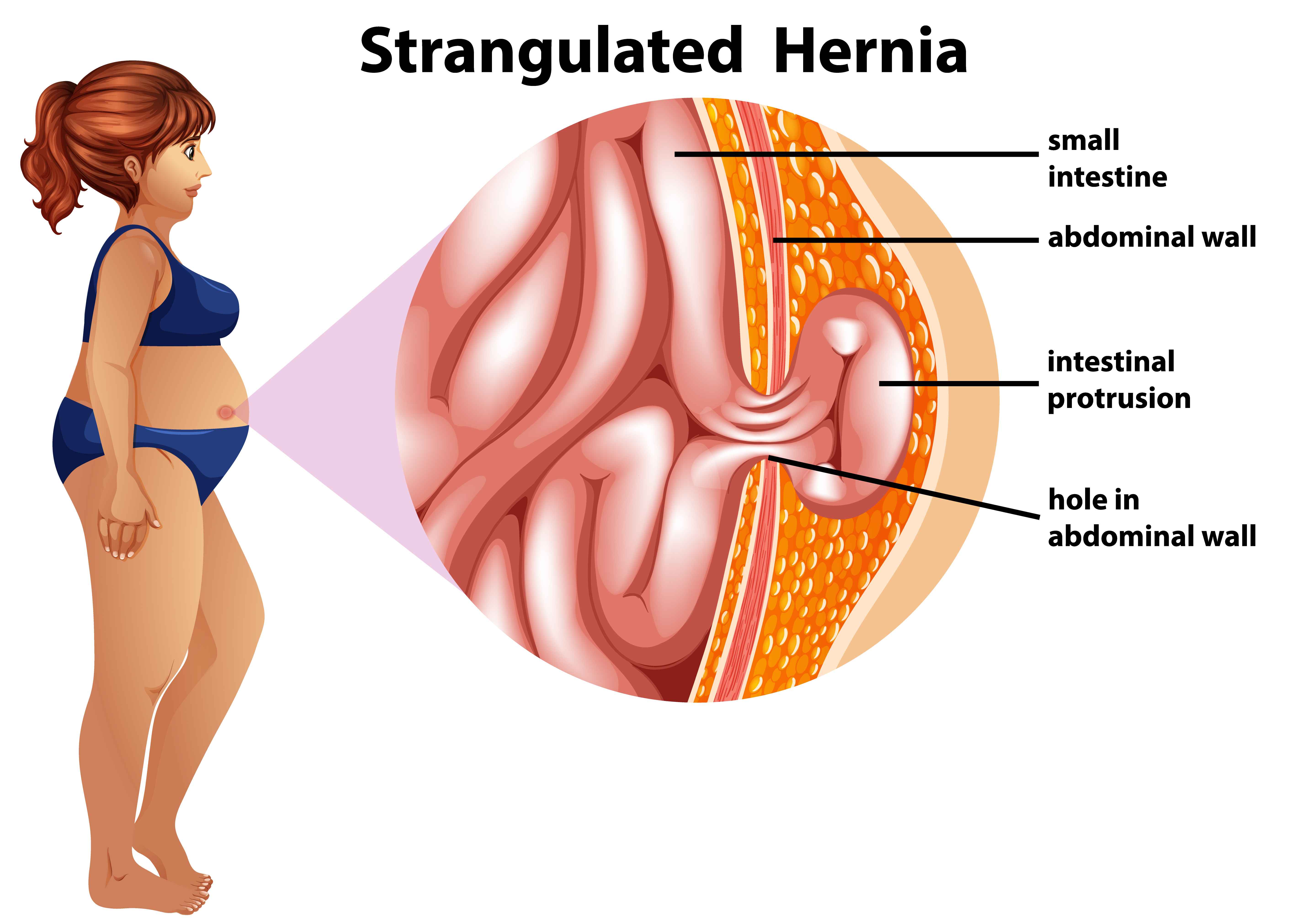
There is no agreement on the best time to have surgery for an umbilical hernia in a pregnant woman or expecting to become pregnant. An emergency repair is unavoidable if the hernia is incarcerated or strangulated at the time of diagnosis. An elective repair should be suggested if the hernia is not complex but causing symptoms.
When the patient has a small and asymptomatic hernia, it may be best to wait until she delivers birth before repairing it. If the hernia is treated just by suture, there is a big chance of recurrence during pregnancy. Umbilical hernia repair during pregnancy may be done with little risk to the mother and the baby.
The second trimester is an ideal time for surgery. Asymptomatic hernias may be treated after delivery or a cesarean section (C-section). Elective repair after delivery is achievable as early as the eighth week postpartum. A one-year interval may provide the patient with a reasonably smooth recovery, including hormonal stability and resumption of normal body weight.
Umbilical Hernia In Women
Women are more likely than males to have umbilical hernias. Because of the steadily growing intra-abdominal pressure, pregnancy may produce an umbilical hernia or make an existing one visible. Most individuals have hernia symptoms throughout the second trimester.
A hernia might be discovered during the first, second, or third pregnancy. In a recent large series, the incidence of an umbilical hernia in pregnant women was as low as 0.08 percent. However, complex instances such as a full-term pregnancy in umbilical hernia, peritonitis owing to skin ulceration, or an imprisoned pregnant uterus inside the hernia rims might occur.
There is no clear surgical protocol for a pregnant lady with a hernia, although more and better scientific evidence has been accumulated.
There is no agreement on the best time to have surgery for an umbilical hernia in a pregnant woman or expecting to become pregnant. In reality, these two sorts of situations should be treated individually. Hernias that are symptomless or have limited symptoms, such as slight discomfort or pain, can be evaluated regularly and treated electively after birth and uterine involution. It has recently been shown that watching and waiting, even for up to 5 years, seems safe for ventral hernias in the adult population.

Umbilical Hernia Before Pregnancy
The correct repair treatment for an umbilical hernia in a woman planning a pregnancy is likewise unknown. Mesh repairs have been demonstrated to be more effective than suture repairs.
WAn elective repair should be recommended if the hernia is symptomatic but not complex. During pregnancy, the larger uterus pulls the intestinal loops to the abdominal cavity's superior and posterior regions. Repairing with simple sutures may result in a recurrence of the condition during pregnancy. Pregnancy following umbilical hernia surgery is independently related to ventral hernia recurrence, and the mesh does not reduce this risk.
An emergency repair, particularly during the first or third trimester, will need anesthetic and surgical trauma. Before planning a pregnancy, it should be suggested that people with significant hernias receive a final repair.
Unfortunately, there is insufficient information about the appropriate gap between hernia repair and pregnancy or delivery. Typically, surgeons tell patients that pregnancy is not permitted for one year after surgical repair. However, there are no clinical or experimental investigations on this instance. There is no unanimity about whether this one-year period ends with the commencement of pregnancy or at the time of delivery. A premature pregnancy is only capable of causing recurrence.
Every hernia brings the danger of imprisonment and suffocation. Patients with an umbilical hernia contemplating pregnancy should be informed of this danger. No one can anticipate which hernias will progress or when they will occur. However, every surgeon can tell their patient about the harmful repercussions of an incarcerated or strangulated hernia on the mother and the unborn child. An emergency repair, particularly during the first or third trimester, will need anesthetic and surgical trauma. Before planning a pregnancy, it should be advised that patients with extensive hernias, including intestinal loops, umbilical hernias with a proa complexity of incarceration, and recurring umbilical hernias previously fixed with mesh have a final repair.
Umbilical Hernia During Pregnancy
When pregnant women should have surgery to repair an umbilical hernia varies. At the time of the diagnosis, an emergency repair will be required if the hernia is incarcerated or strangulated. An elective repair should be suggested if the hernia is not complex but does cause symptoms.
When the patient has a little hernia that is not causing any symptoms, it is possible that delaying the surgery until after she gives birth is the best course of action. If the hernia is treated with sutures alone, there is a significant possibility that it may return when the patient is pregnant.
It is possible to repair an umbilical hernia during pregnancy with a slight risk to the mother or the unborn child. The second trimester is an appropriate time for surgical intervention. Asymptomatic hernias may be corrected either after delivery of the baby or at the time of a cesarean section (C-section).
Umbilical Hernia Repairing During C-section
Repairing a hernia during a cesarean section is a standard surgical technique. At the moment of C-section delivery, it is possible to correct umbilical hernias. The combination C-section and hernia repair procedure have a high success rate in making patients happy. On the other hand, an increased incidence of recurrence is to be anticipated. The time required for combined procedures to repair an umbilical and an inguinal hernia is longer than necessary for a C-section alone. However, there was no evidence of a recurrence after the procedures were performed. Consequently, combination surgical procedures are risk-free and reduce the need for readmission.

Umbilical Hernia After Childbirth
Some pregnant women with umbilical hernias do not have hernia repair done simultaneously with the C-section. The cause for this might be a patient or surgeon's preference. Pregnant individuals with reducible groin or umbilical hernias may be successfully handled non-operatively throughout pregnancy and then receive surgical correction in the postpartum period. Although umbilical hernia repair is possible after delivery, surgery on small asymptomatic hernias in the early postpartum period is unnecessary. A one-year interval may provide the patient with a reasonably smooth recovery, including hormonal stability and resumption of normal body weight. If the patient wishes to have additional children, surgery may be postponed for longer, even after another pregnancy.
Complications Associated With Hernia Repairing During Pregnancy
Following are some of the possible risks of hernia repair during a C-section.
Muscles And Fascial Structures Changes
The rectus abdominis muscle's general anatomy changes during pregnancy. Muscle length, separation, and insertion angle grow significantly as the pregnancy progresses. The abdominal muscles' functional capacity is also changed, as is their ability to maintain the pelvis.
Upper rectus abdominis relative integrated electromyography (EMG) rose throughout all abdominal workouts, but external oblique and lower rectus abdominis relative integrated EMG declined. By 18 weeks post-birth, relative EMG for all examined muscles had reverted to values found at 18 weeks and 26 gestations.
Functional alterations were discovered in the rectus abdominis and the external and internal obliques. Separation of the rectus abdominis was corrected by 4 weeks post-birth, and abdominal muscle inter-relationships were restored to pre-pregnancy levels by 8 weeks post-birth.
However, at 8 weeks after delivery, the capacity to maintain the pelvis remained poor. This persistent decrease in the ability to support the pelvis 8 weeks after delivery might be attributed to the inadequate resolution of abdominal muscle length increases caused by pregnancy.
Relaxin
Hormonal changes during pregnancy may also impact the outcome of hernia repair in a pregnant or early postpartum woman. Relaxin is an insulin-like peptide hormone released by the corpus luteum. During pregnancy, it is also secreted by the placenta. It softens and expands the cervix while relaxing pelvic ligaments.
Relaxin inhibits the formation of the extracellular matrix (ECM) and promotes collagen breakdown. Relaxin significantly reduced tissue collagen levels in rats in research. Relaxin inhibited collagen formation while increasing collagen breakdown. Any endogenous or exogenous chemical that interferes with these systems may reduce recurrence after hernia surgery, particularly after suture repairs.
When the repair is completed, and the relaxin level is high, there is a chance of recurrence. Relaxin may potentially have a role in developing perineal hernias in dogs with connective tissue degeneration. There is just one report on humans' relationship between relaxin and abdominal hernias.
Would Carrying Baby Cause Damage?
Following hernia procedures, patients are usually restricted from lifting weights. Even mesh repairs are susceptible to intra-abdominal pressure elevations in the early postoperative period. According to biomechanical tests, the tensile strength produced by tissue ingrowth into the mesh reaches roughly 80% after just 6 weeks.
Although there is no agreement on weight lifting restrictions after hernia operations, surgeons advise their patients not to lift any weight for the first two weeks. After 2-4 weeks, light lifting (up to 10 kg) is permitted. Patients are recommended to lift more than 10 kg after 8 weeks.
In reality, carrying and raising a newborn would be within the guidelines. A lady with no kid and an umbilical hernia repaired will be restricted from lifting weights for a significantly extended period.
People Also Ask
When Should I Be Concerned About An Umbilical Hernia?
If your kid still has the hernia after reaching 5 years old, you should make an appointment with the doctor. You should call your doctor immediately if the hernia becomes bigger, seems puffy, or is challenging. Your child's hernia protrudes while sleeping, at ease, or laying down, and you can't shove it back in.
How Is An Umbilical Hernia Treated During Pregnancy?
Minor laparoscopic surgery with tiny incisions may be required to correct it. Less severe instances may be postponed until after the baby is born, but your doctor may potentially conduct surgery during pregnancy (usually in the second trimester). During a C-section, an umbilical hernia may potentially be surgically repaired.
What Happens If You Have An Umbilical Hernia While Pregnant?
When the patient has a small and asymptomatic hernia, it may be best to wait until she delivers birth before repairing it. If the hernia is treated just by suture, there is a big chance of recurrence during pregnancy. Umbilical hernia repair during pregnancy may be done with little risk to the mother and the baby.
Conclusion
There is no agreement on the best time to have surgery for an umbilical hernia in a pregnant woman or expecting to become pregnant. An emergency repair is unavoidable if the hernia is incarcerated or strangulated at the time of diagnosis. An elective repair should be suggested if the hernia is not complex but causing symptoms.
If the hernia is treated with sutures, the chance of recurrence during pregnancy is significant. Mesh repair may limit the flexibility of the abdominal wall and induce discomfort during a future pregnancy. When the patient has a small and asymptomatic hernia, it may be best to wait until she delivers birth before repairing it.

Karan Emery
Author

Katharine Tate
Reviewer
Latest Articles
Popular Articles