Astrocyte - What Role It Can Play In Intellectual Disability
Understanding the astrocyte process in intellectual development disorders can aid in creating novel therapeutic targets for treating intellectual disability-related illnesses.
Author:Katharine TateReviewer:Karan EmeryOct 09, 202322.8K Shares309.2K Views
Intellectual disability is a form of neurodevelopmental illness caused by a malfunction in the nervous system.
Its occurrence is strongly linked to neurological development. Astrocytesare the most abundant cells in the mammalian brain.
Research has shown that astrocytes only support and separate neurons in the brain. They also play a vital function in brain development.
Understanding the astrocyte process in intellectual development disorders can aid in creating novel therapeutic targets for treating intellectual disability-related illnesses.
Astrocytes - for beginners
What Is Intellectual Disability?
Intellectual disability is a neurodevelopmental condition that causes severe impairments in intellectual and adaptive functioning.
It is characterized by an IQ of less than 70 and deficiencies in two or more adaptive behaviors that influence daily public life.
DSM-V defines intellectual functioning as reasoning, problem-solving, planning, abstract thinking, judgment, academic learning, and learning through instruction and experience, as well as practical understanding as proven by clinical evaluation and standardized testing.
Adaptive behavior is characterized in terms of intellectual, social, and functional abilities concerning daily activities undertaken by humans.
Intellectual disability is classified as syndromic intellectual disability, which occurs in conjunction with other medical and behavioral signs and symptoms, and non-syndromic intellectual impairment, which occurs in the absence of other abnormalities.
Syndromic intellectual impairments include Down syndrome and Fragile X syndrome.
About 2 to 3% of the population is affected by intellectual impairment.
Approximately 75 to 90% of those afflicted have a minor intellectual handicap. 30 to 50% of these instances are non-syndromic or idiopathic.
A genetic issue causes around a quarter of cases, and about 5% of patients are inherited from one's parents. As of 2013, over 95 million individuals were affected by cases of unclear etiology.

Astrocytes Role In Intellectual Disability
Intellectual disability is caused by many factors, which can be divided into genetic and environmental.
Several diseases, including Down's syndrome and Fragile X syndrome, are caused by neuronal changes.
Astrocytes are closely associated with the development of neurons and may play an important role in intellectual disability.
Malnutrition, brain trauma, maternal, perinatal infection, and early childhood central nervous system infection may cause intellectual impairment.
Intellectual Disability Caused By Reactive Astrocytes
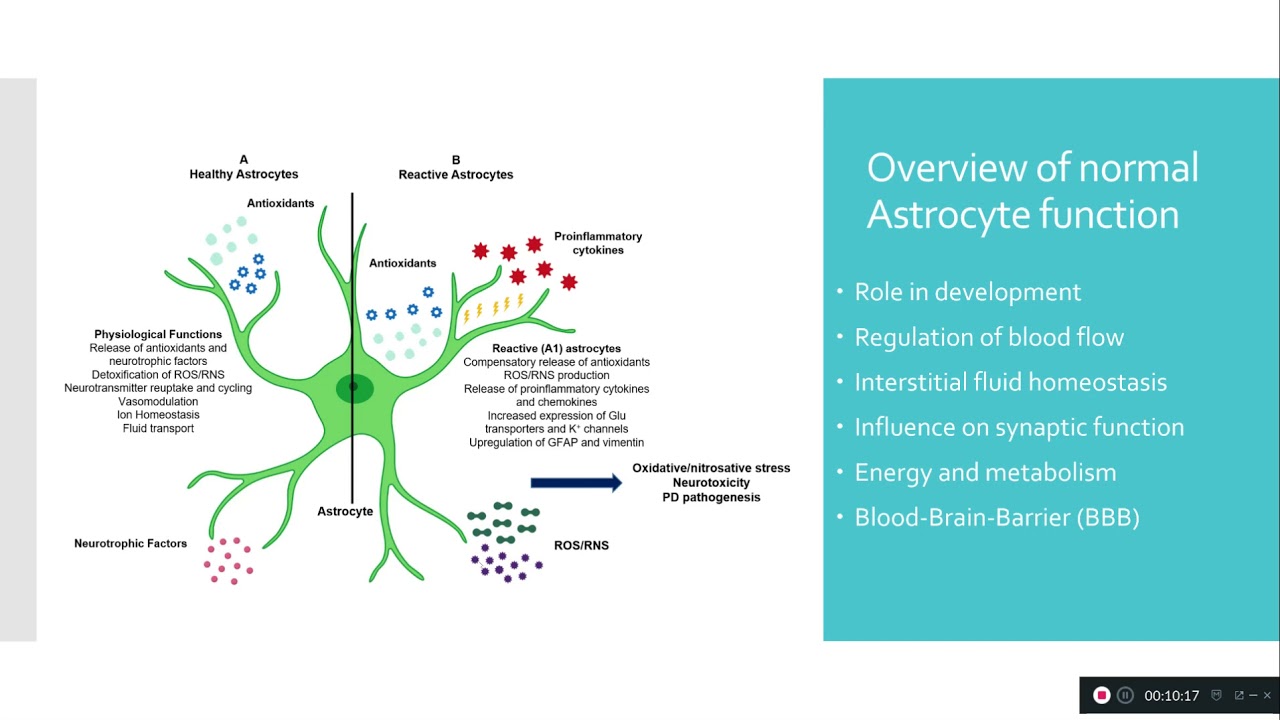
When the nervous system is harmed or pathological changes occur, astrocytes react by releasing numerous chemicals within and outside the cells, resulting in haemostatic, morphological, and functional alterations.
These modifications will cause an inflammatory response that will disrupt central nervous system homeostasis by limiting normal neuron development or death.
Increased reactive astrocytes in intellectual disability-related disorders often have negative consequences on the central nervous system, manifesting in the inflammatory response.
The inflammatory response was also detected in a Down's syndrome mouse model.
Intellectual Disability Caused By Ion Channel Dysfunction Of Astrocytes
In addition to the inflammatory response, astrocytes have many effects on neuronal ion homeostasis in various intellectual disability-related diseases.
In the tuberous sclerosis model, the expression of K+ channels and other ion channels is reduced, which will decrease their ability to buffer potassium.
A series of changes will eventually result in the overexcitation of neurons, leading to a tuberous sclerosis complex.
Astrocyte ion channels, such as the K+ channel, BEST-1, and hemichannels, contribute to neurodevelopmental disability and intellectual disability.
An imbalance between glutamate and GABA in FXS astrocytes produces neurotoxicity, shortening neuronal dendrite lengths.
The expression of glutamate transporters such as GLAST and GLAST also decreased in the tuberous sclerosis model.
In the Rett syndrome model, the metabotropic glutamate receptor 5 expressions and Ca2+ response were decreased, weakening the expression of neuron-dependent GLT1 and eventually reducing the neuronal glutamate uptake.
Increased extracellular glutamate levels lead to central nerve cell death and impaired synaptic plasticity and learning due to excitotoxicity.
Some studies on disease models have found that reactive astrocytes can protect neurons against central nervous system damage.
Astrocytes' Molecular Dysfunction in Intellectual Disability
Reduced brain-derived neurotrophic factor in astrocytes may be one mechanism contributing to aberrant neuronal development in the Rett syndrome model.
The number of calcium-binding presynaptic proteins, synaptophysins, and postsynaptic scaffold proteins, PSD95, located at the neuronal synapses is reduced due to coculture.
In the Down's syndrome model, persistently elevated S100 expression will raise ROS generation, activate the stress response kinase, and cause cell death.
A crucial secretory protein that aids in controlling spinal growth and synaptic formation is thrombospondin-1 (TSP-1).
Astrocyte Dysfunction In Intellectual Disability Linked To Environmental Factors
A pregnancy-related infection will also influence the development of astrocytes and neurons, leading to intellectual disability and, ultimately, neurodegenerative disorders.
The increased serotonin receptor sensitivity in the offspring of pregnant rats raises the risk of neurological disorders.
Ethanol may decrease serotonin in the mouse brain and lead to intellectual disability.
Experiments involving in vitro exposure to lead indicate that Pb may activate astrocytes, stimulate the production of inflammatory factors, and induce an inflammatory response.
It may also cause oxidative stress in astrocytes and inhibit the astrocyte cell cycle.

Intellectual Disability
Intellectual Disability Drugs And Astrocytes
There have been five ways of intellectual disability management: physical, training, psychological, nutritional, and medication treatment.
Multiple medications, including piracetam, aniracetam, monosialotetrahexoylganglioside sodium (GMI), mecobalamin, vitamin B12, and methylphenidate hydrochloride, have been used to treat mental illnesses.
Medications containing cetam may counteract the impact of scopolamine on glucose utilization in the cerebral cortex.
After therapy with piracetam, mitochondrial ATP generation and membrane potential were increased in an Alzheimer's disease model, which decreased apoptosis and promoted neural plasticity.
Studies have shown that cetam medicines can both slow down the deactivation of the AMPA receptor and raise the calcium concentration in astrocytes.
Slowing the AMPA receptor deactivation may also block the potassium current in astrocytes by raising endogenous Na+ levels, protecting against neuronal overexcitation-induced toxicity.
Additionally, cetam medicines may decrease oxidative stress damage in astrocytes, as well as GFAP and astrocyte reactivity, helping enhance patients' memory and brain function.
Monosialotetrahexosylganglioside sodium (GMI) is an essential component of mammalian nerve cells and can partially prevent the abnormal release or reuptake of excitatory amino acid neurotransmitters such as glutamate; consequently, it can avoid excessive glutamate expression from causing damage to brain nerves and tissues.
GMI may also enhance cerebral blood circulation, boost blood oxygen, protect neurons, and diminish N-methyl-D-aspartate-dependent excitotoxicity caused by morphological astrocyte enlargement.
Vitamin B12 was required for nerve growth. Increased reactive astrocytes were seen in the grey matter of rats low in vitamin B, with microglial oedema and myelinolytic lesions.
Mecobalamin and vitamin B12 may supplement vitamin B12 in the brain; stimulate nucleic acid and protein synthesis; enhance axonal transport, axonal regeneration, and myelin production to avoid axonal degeneration; heal damaged nerve tissues, and improve the brain's damaged glial cells.
Intellectual Disability Levels
Based on your child's IQ and level of social adjustment, intellectual impairment is classified into four stages.
Mild Intellectual Disability
Mild intellectual impairment symptoms include the following:
- It takes them longer to learn to speak, but once they do, they communicate effectively.
- becoming completely self-sufficient in self-care as they age
- having difficulties with reading and writing
- immature social behavior
- greater trouble with marital or parental obligations
- taking advantage of specialized education programs
- with an IQ ranging from 50 to 69
Moderate Intellectual Disability
Your kid may experience some of the following symptoms if they have moderate ID:
- are sluggish to comprehend and use language
- may encounter communication challenges
- can develop fundamental reading, writing, and counting abilities
- are often unable to live on their own
- can often go about on their own to known locations
- may participate in a variety of social activities
- having an IQ ranging from 35 to 49
Severe Intellectual Disability
Severe ID symptoms include:
- visible motor impairment
- Their central nervous system has suffered severe harm or has developed abnormally
- having an IQ ranging from 20 to 34
Profound Intellectual Disability
Among the symptoms of severe ID are:
- failure to comprehend or follow requests or directions
- potential immobility
- incontinence
- nonverbal communication at its most fundamental
- incapacity to care for their own needs on their own
- the need for ongoing assistance and monitoring
- having an IQ lower than 20
Intellectual Disability Diagnosis
Your kid must have below-average intellectual and adaptive abilities to be diagnosed with an intellectual disability.
Your child's doctor will conduct a three-part assessment, which will include standard exams, discussions with you, observations of your kid,
Standard intelligence tests, such as the Stanford-Binet Intelligence Test, will be administered to your kid. This will assist the doctor in determining your child's IQ.
The doctor may administer other tests, such as the Vineland Adaptive Behavior Scales.
This exam compares your child's daily living skills and social talents to those of other youngsters their age.
It is important to note that children from various cultures and socioeconomic backgrounds may perform differently on these examinations.
Your kid's doctor will evaluate the test findings, discussions with you, and observations of your child when making a diagnosis.
Your child's assessment procedure may involve visits to professionals such as a speech pathologist, psychologist, social worker, developmental pediatrician, physical therapist, or pediatric neurologist.
In addition, laboratory and imaging studies may be conducted. These may aid your child's doctor in detecting metabolic and genetic diseases and structural issues with their brain.
Other issues that might cause delayed development include hearing loss, cognitive impairments, neurological abnormalities, and emotional problems.
Before diagnosing your kid with ID, your child's doctor should rule out these disorders.
You will use the findings of these tests and assessments of the child's school and your doctor to establish a treatment and education plan for your kid.
Vineland Adaptive Behavior Scales | Psychology | Iqra Sageer
People Also Ask
What Are The 4 Levels Of Intellectual Disability?
- Profound
- Severe
- Moderate
- Mild
What Are The Most Common Intellectual Disabilities?
The Top 5 Types of Intellectual Disabilities
- Autism. Autism is a developmental disorder that affects the neurological system as well as the structure and function of the brain.
- Down's Syndrome
- The Fragile X Syndrome
- Fetal Alcohol Syndrome (FAS)
- The Prader-Willi Syndrome (PWS)
What Are Three Signs Of Intellectual Disability?
- Youngsters sit up, crawl, or walk later than normal children.
- Learn to speak later or have difficulty speaking
- Have trouble remembering stuff.
- Have difficulty grasping social norms
- Having difficulty comprehending the consequences of their actions
- Have difficulty addressing issues
What Is Considered An Intellectual Disability?
Intellectual disability (or ID) is a term used to describe a person with difficulties in cognitive functioning and abilities such as communication, social, and self-care.
Because of these constraints, a kid may grow and learn more slowly or differently than a normally developing youngster.
Final Words
In recent years, astrocytes' involvement in cerebral development has been steadily uncovered via in-depth study.
Their alterations are also intimately linked to the onset and course of several neurological disorders.
The etiology of intellectual disability is complex, and many of its processes remain unknown.
Consequently, this mini-review demonstrates that functional alterations of astrocytes under the influence of numerous pathogenic causes are strongly associated with intellectual disability and that various medications for intellectual disability may also reduce astrocyte lesions to variable degrees.
To treat intellectual disability-related disorders, a few effective drugs have been supplied for functional alterations of astrocytes under pathological situations.
This indicates that astrocytes' morphological and functional modifications may be a fundamental mechanism behind these illnesses.
Dissecting the contribution of diverse astrocyte subtypes to disorders associated with intellectual disability might give a viable treatment strategy and assist these individuals.
Consequently, medicines that block astrocyte lesions may emerge as a novel and effective therapy for intellectual disability in the future.

Katharine Tate
Author

Karan Emery
Reviewer
Latest Articles
Popular Articles